Note: This is Part 2 of ‘Politics and economics explained’, an assignment happily entered into for my immediate family and made freely available here to others. The narrative is made more accessible to non-economists as a result of its unreliability and through the addition of references to a number of films which relate to the piece’s subject areas. Part 1 was ‘1940-1960’ and is available on this same blogg.
The scariest thing about living during the Cold War was the possibility of a nuclear war between the Soviet Union and the US. Back then it seemed possible that one or other of those countries might somehow get an unhinged leader who could order a nuclear attack on the other superpower. [Dr. Strangelove. 1964]
By 1960 people seemed to have forgotten the value of having a government lead on commercial activity, and suddenly the only thing that mattered was the profitability of commercial enterprises. When Dr Beeching took over as Chairman of the British Transport Commission in 1964, British Rail was losing £140 million a year. So he closed 4,500 miles of railway line and 2,128 stations. This was one third of the track network and 55 per cent of stations, or the equivalent of six extra seasons of Michael Portillo’s Great British Railway Journeys (on BBC2). These closures led to the loss of 67,000 British Rail jobs – a sort of dress-rehearsal for what was in store for much of the UK’s heavy industry.
Soon
after Beeching’s closures people thought they could see light at the end of the
tunnel. Unfortunately it turned out to be a train coming in the opposite
direction. This was the thundering, unstoppable neoliberalism, a new fashion
for western governments that was to dominate politics and economics for half a
century and wasn’t really challenged until there was an unexpected viral
pandemic.
Neoliberalism
was invented by Milton Friedman in Chicago one day in 1967 – and we’re still
trying to get over it today. Friedman said that not only was it a bad idea to
have governments do stuff, but that government intervention actually does harm. When the economy is slowing down and
unemployment rising, the government should sit on its hands and let the central
bank manage growth by increasing the amount of money in circulation. This will reduce interest rates and increase
spending. (This is ‘monetarism’.)
People were persuaded. After 20 years of controlled economic expansion in which government investment (especially by the US) played a leading role, governments everywhere – Conservative, Liberal, Labour – signed up to ‘monetarism’ and turned their backs on Keynes. [Capitalism: A Love Story. 2009]
Monetarism is a central tenet of neoliberalism which has a particular view of the relationship that a government should have with its people. It holds that free-market capitalism is all the go. It sees competition as the best characteristic of human relations. We are all consumers, not citizens. All of our choices and behaviours and attitudes are best exercised by buying and selling, a process that rewards merit and punishes inefficiency. ‘The market’ delivers benefits that can’t be achieved by planning and ensures that everyone gets what they deserve. Inequality is a sign that things are working well. [Suits. 2011-19]
The successes of neoliberalism include the financial meltdown of 2007‑8,
the Panama Papers, the slow collapse of public health and education, resurgent
child poverty, the epidemic of loneliness, the collapse of ecosystems, and the rise
of Donald Trump. [The Laundromat. 2019]
[Sorry We Missed You. 2020]
One of the best practitioners of neoliberalism was Margaret, Baroness Thatcher, Prime Minister of the United Kingdom from 1979 to 1990. She loved markets and put structural change in the UK economy on steroids by closing all the coalmines and steelworks. She also had a wapping victory over print unions and helped Rupert Murdoch buy news organisations and salacious newspapers. [Hack Attack. date tbc] [My Beautiful Laundrette. 1985.]
PM Thatcher famously said there is no such thing as society:
I think we’ve been through a period where too
many people have been given to understand that if they have a problem, it’s the
government’s job to cope with it: ‘I have a problem, I’ll get a grant.’ ‘I’m
homeless, the government must house me.’ They’re casting their problem on
society. And, you know, there is no such thing as society. [High Hopes. 1988.]
Between 1984 and 2014 over a quarter of a million coal miners in the UK lost their jobs. In 2014 there were still 5.5 million people in ‘coal mining regions’ who needed financial support. The steel industry was similarly affected. The UK steel industry employed 323,000 people in 1971, but 32,000 in 2019. The fracturing of local communities had serious adverse effects on a whole range of communal activity, including sporting clubs and local orchestras, but these were offset for some people by increased employment opportunities in male strip shows. [Brassed Off. 1996] [The Full Monty. 1997]
From
1997 to 2003 there is stable and fun government in the US. The leader of the
Western world and his staff grapple in entertaining fashion with tough issues
like modernisation of the US polity, religious fundamentalism, terrorism and
the politics of the Middle East. [TheWest Wing. 1999-2006]
However in response to terrorist attacks on the US, in 2003 President Bartlett’s successor led the United States into war in Iraq. The aims were to punish the Iraqi President for the use of chemical or biological weapons of mass destruction, to install a pro-US government there and to dissuade it and other countries in the Middle East from shielding terrorist organisations. The US was joined in the operation by Australia and the UK. The Iraq War lasted seven years, saw 4,488 U.S. troops killed and cost the US over a trillion dollars. In comparison, World War 2 cost the US $4.1 trillion (inflation-adjusted) and the Vietnam War $738 billion. [Good Morning, Vietnam.1987] [Platoon. 1986]
In the UK, 1997-2010 is a period of faux socialism during which social-democratic and neoliberal policies and approaches are pretty much indistinguishable. Then, in 2010, David Cameron (a Conservative) becomes the youngest Prime Minister since Lord Liverpool in 1812. As Prime Minister he has two good moments. The first was when he became uncharacteristically firm in negotiations with the US President when he (the President) was caught coming on to his girlfriend. [Love Actually. 2003] The second was when he inexplicably decided to hold a referendum (June 2016) into the UK’s membership of the European Union. [Brexit: The Uncivil War. 2019]
Despite
ample evidence from The West Wing, the Panama Papers and a global financial crisis, neoliberalism
is still unchallenged as the preferred paradigm for governments throughout The Developed
World. It succeeds in reinventing itself time and again through ephemeral
schemes like subprime mortgages and less ephemeral ones like the sudden stupendous
wealth of Russian oligarchs. All of this means that, in 2016, even someone like
a 59-year-old carpenter who has had a heart attack has to fight bureaucratic
forces in order to get unemployment benefit. [I,
Daniel Blake. 2016] [The Era of
Neoliberalism. 2019]
It’s as if the world’s economic order is waiting for some unstoppable natural phenomenon to jolt it into the realisation that it needs to Make Kindness Great Again.
Mathematical models of disease transmission can be used to estimate the potential impact of public health responses to infectious diseases. Recently (7 April) some details of the particular model that is being used as the basis for the decisions of Australian governments on the COVID-19 crisis have been published.
How do such models work? How can we be sure they are accurate? What do they tell us?
The headline findings from the modelling are the ones that have been delivered to us consistently in governments’ media conferences and other information activities:
An uncontrolled COVID-19 epidemic would result in a situation dramatically exceeding the capacity of the Australian health system over a prolonged period, notwithstanding the increases in that capacity that are possible.
A combination of case-targeted isolation measures with general
social measures will substantially reduce transmission and result in a more prolonged epidemic with lower peak incidence, fewer overall infections and fewer deaths.
As we all know, we have to stay home.
How it works
These general prescriptions from the modelling are clear and largely unchallenged. But as time passes it will be good if there is closer scrutiny of this and other modelling. This will result in better understanding of both the general applicability of such modelling and the specific work being done on the Australian government’s preferred model.
The key variables on which mathematical models of infection are based are the latent period (i.e. the interval following exposure before an individual becomes infectious and transmits the disease), the infectious period (i.e. the period during which an infected person can transmit a pathogen to a susceptible host), and transmissibility. Transmissibility is described by the reproduction number – the number of secondary cases generated by a single infected case introduced into a susceptible population.
If the transmissibility number is less than 1, infection is receding. If it’s greater than 1, infection is spreading.
For models of this kind it is useful to know the extent to which outputs (in effect, the model’s predictions) change in response to a given amount of variation in its inputs, and the particular input to which altered outputs can be attributed. The inputs include both the assumptions made about the structure of the entity being modelled and the data fed in.
This is the business of uncertainty and sensitivity analysis. In effect they provide information about the robustness of the model – the probability of the model and its predictions being accurate reflections of reality. The greater the model’s uncertainty or sensitivity, the more its outputs change with a given amount of variation of its inputs – and the less useful it will be.
Such analyses can help check the accuracy of a
model’s structure or specification by assessing the individual contribution of
a variable and the need to include it or not.
They can also help interpret the results of a model
by identifying thresholds for certain variables that trigger outcomes of
interest.
The value of any such modelling is limited if the model’s structure is imperfect (that is, if it makes false assumptions about the relationships between elements of the model) or if incomplete or inaccurate data are fed into it. The modelling can be run again and again with greater confidence about its accuracy as, each time, more is known about the characteristics of thepathogen and more local (Australian) data are added in.
Critically, accurate estimation of the transmissibility of a disease requires reliable data on its incidence in the total population. As we have been told time and time again, this requires “testing, testing and testing”.
In addition to the latent period, the infectious period and
transmissibility, more specific variables can be included in the model, such as
the structure of the population and its mobility patterns, demographic
variables, risk factors and age profiles. But with every new variable included
the risk of false assumptions or imperfect data is likely to increase.
The preferred Australian model for use with COVID-19
There are a number of mathematical models doing their stuff around the world on the spread of infectious diseases and the impact of various public health responses. The one that has been, and remains, the basis for the decisions of Australian governments on the COVID-19 crisis is managed by the Peter Doherty Institute for Infection and Immunity, a joint collaboration of the University of Melbourne and the Royal Melbourne Hospital.
The Doherty team released to the public a paper on 7 April
2020 about their modelling work on COVID-19.
The paper is quite open about potential weaknesses of the
model that stem from unavoidable uncertainties about the assumptions made and imperfect
or incomplete data relating specifically to the progress of the disease in
Australia. Since it is a new pathogen there are uncertainties about the true
disease ‘pyramid’ for COVID-19, and a lack of information about determinants of
severe (as distinct from mild) disease. In the modelling done so far, age has
been used as a best proxy for the probability of symptoms becoming severe.
There are other uncertainties. The model being used has been converted from one used for influenza and there are great differences between that pathogen and COVID-19. The assumptions about reducing transmission of influenza through a combination of distancing measures come not from Australian data but from Hong Kong. The relative contributions of different measures, such as the cancellation of mass gatherings, distance working, closure of schools or cessation of non-essential services, are not yet clear.
More will be learned about these particular strategies from real time data now being collected by various Australian agencies. In turn this will enable the more precise estimation of transmissibility for COVID-19 in Australia. This will be used to update forecast trajectories of the epidemic. These will no doubt be among the key pieces of information used by governments to manage the ongoing responses to the pandemic.
Some critical unknowns
Perhaps the most serious and alarming reminder in the published paper is that low and middle-income countries will find it even harder – potentially quite impossible – to deal with the COVID-19 crisis. Their health systems are already weaker, with limited access to high level care.
Given the massive impact on world trade and damage to the budgets of all countries, including those that are affluent that have been donors of international aid, the impact of the COVID-19 emergency on the people and governments of poorer countries may become quite unmanageable.
Much will depend on the role played by international aid and
trade in the new order.
One of the most critical omissions from Australia’s modelling to date is that it has not as yet accounted for the loss of health care workers due to illness, carer responsibilities or burnout. Nor has it accounted for shortages of critical medical supplies, because the true extent of these shortages and their likely future impacts on service provision are apparently still unknown.
These are two aspects of the issue to which governments and
others must continue to give urgent attention. Apart from anything else it
reminds us of the very special place of health care workers and the risks they
face. Let’s continue to applaud, thank and support them.
Uncertainty and sensitivity analyses may perhaps already have been used by the team in Melbourne to investigate any number of aspects of the modelling. For example the published paper reports that in the simulation of a case-targeted public health intervention it was assumed that 80% of the identified contacts adhered to quarantine measures. It would be useful to know how many additional ICU beds would be required if the compliance rate was 78% or 82%, for example.
With the publication of the Institute’s paper a start has been made down the track of ensuring that the public becomes more familiar with, and more trusting of, the basis of many of the decisions affecting them. It will help to equip the Australian people for the kinds of generous and determined responses that will be needed for global recovery.
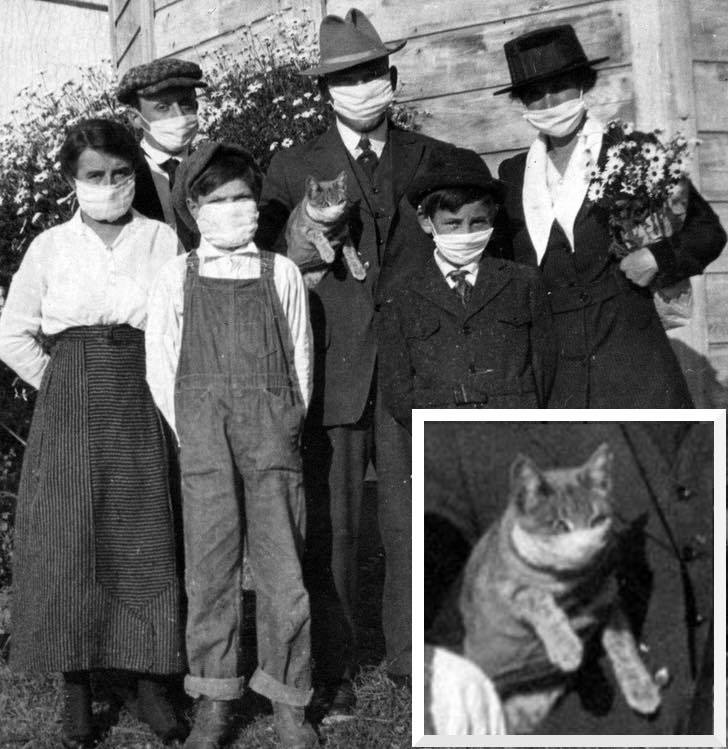
It seems odd that there has been no clear
and unequivocal advice about whether or not it would help if we all wore face
masks. This piece considers the many different aspects of the question which,
between them, explain its complexity and why there has not yet been a single clear
recommendation. Instead the matter has been left to individuals to decide.
This organic approach to an issue in which every one of us is potentially involved has at least two advantages. It lets the authorities off the hook of accountability for any sort of uniform advice. And it cedes responsibility to the people, which is widely considered a desirable principle. But if and when there is a clear technical (health or clinical) case for a particular protocol relating to masks, it will be an important challenge for the authorities to spread the word and obtain widespread community compliance.
“Who was that masked man?”
School
closures
Two weeks ago the question of whether
or not schools should be closed seemed to be the most critical on which there
was no clear advice. The experts had discussed the matter. We were told that
schools would remain open but it would be good if parents who were able to do
so would keep their kids at home.
The solidarity of the National Cabinet
seemed to be fractured. Different jurisdictions provided different advice,
based not just on medical views but on logistical matters such as when school
terms were ending. Very soon it became apparent that the matter was apparently
too complex for uniform national action to be agreed and it fell to parents to bear
responsibility for the decision.
This cannot be seen necessarily as a
criticism or failure of ‘the powers that be’. It may well be that the mixed
mode that emerged about schools was in fact optimal given all the relevant
circumstances and considerations.
The characteristics of that decision on schools which made it so complex seem now to relate to the question of whether or not to recommend or potentially even to mandate the wearing of masks. Is it to be Tonto or the Lone Ranger?[1]
Aspects of the question
Where the wearing of masks is
concerned, the aspects to be considered include the following.
1. Does the wearing of masks reduce
rates of transmission? This might appear to be the simplest and most important
question but, even without scientific knowledge, one can understand its
complexity. It obviously depends on the number, type and location of mask
deployed. Does the effectiveness of masks depend on the proportion of the
population who wear them? Why does the evidence from other countries seem to be
conflicting? One thing that is clear is that masks are effective only when used in combination
with other measures, most particularly frequent hand-washing with soap and
water. The efficacy of masks is impacted by their supply; in short
supply, the risks multiply of having them used in an unhygienic fashion.
2. Does the wearing of masks have
desirable or undesirable effect on the extent to which the population, or
particular groups within the population, are compliant with critical measures
like self-isolating and social-distancing? Some have argued that people wearing
masks, or seeing others wear them, instils over-confidence and a lack of the
required discipline on other fronts. The widespread use of masks could
conceivably increase the public’s pessimism and propensity for
‘catastrophisation’. This could have adverse effects for mental well-being.
3. There is clearly a hierarchy of
need relating to the wearing of masks and other personal protective equipment.
Clinicians and others ‘on the frontline’ must be given first dibs, both for
their own safety and for the effectiveness of the health and related systems.
Any increase in the encouragement of others in the population to wear masks would
therefore have to be moderated by accurate knowledge about the supply of masks.
4. “A mask is not a mask.”
All sorts of products exist, including surgical masks and cloth or
fabric face coverings. Surgical masks and respirators are essential for
practitioners dealing with COVID-19 patients and those suspected of having it. Even
if a uniform decision was possible on other fronts, there would be questions
about what types of mask is useful in particular circumstances. We have seen
and heard much about ingenuity of individual people and retooled companies
making masks, but the efficacy of
various models and their uses has to be considered.
5. Consideration needs to be given to the cultural aspects of wearing masks. In Australia we look to countries to our north to see community/political entities (Singapore and the like) which are more accustomed both to wearing masks and to being told what to do on such matters. To the rugged individualists we are supposed to be, being told to wear masks may be a bridge too far, jeopardising a national consensus.
6. Some will argue that the question
of mandating the wearing of masks is a legitimate battleground on the ‘personal
freedom v. government control’ front.
7. There may be implications relating
to the effect of a uniform approach on particular subgroups of the population.
If wearing masks has cost indications not covered by governments, mandating
their wearing would contribute to further inequality between rich and poor,
employed and unemployed. The same might be said for urban-rural differences and
equity. If there are national shortages of masks and other personal protective
equipment they are certain to be greater and to have more impact in rural and
remote areas than in the major cities.
8. Wearing a mask needs to be done
properly. Any mandatory use of masks would need to be accompanied by detailed
practical advice about what to do before putting it on, when to change it, how
take it off and how to discard it. The WHO and many other organisations provide
essential information about such matters which should be consulted by potential
users. There is a recent article on the issue at https://insidestory.org.au/so-you-want-to-wear-a-mask-in-public/
It might be that, in their wisdom,
governments and their advisers have tacitly agreed that it would be best if the
decision about wearing masks remained organic – something to be owned and
narrated by the community itself, evolving at the pace determined by people
themselves. This would have some of the characteristics of the responses to the
COVID-19 situation advocated by those who trust in citizen engagement and
community development. I belong to that group but also crave information and
advice from technicians about matters that can be subject to technical
certainty.
And the Lone Ranger? Every week after
he and his trusty friend Tonto had saved the world in 30 minutes, they would
ride off into the distance, silhouetted against the skyline. Someone turns to
the sheriff to ask who that masked man was. The sheriff responds that it was
the Lone Ranger, who is then heard yelling “Hi-Yo Silver, away!” as
he and Tonto ride away. We could do with him back again.
Information
and disclaimer: this article has been written in the belief that policies relating
to the wearing of masks are complex and illustrative of the great difficulties
posed for decision makers by the current COVID-19 situation. It is not my
intention to make or promote judgements about the clinical, social or economic
aspects of the matter and it is certainly not my intention to provide advice to
individuals. There is a mass of information online about the wearing of masks
in the current situation and people making a personal decision should consider
that information.
Some circumstances make the wearing of
a mask essential. They include the situation in which a patient is suspected of
having infection or when someone is coughing or sneezing such that a physical
barrier between them and another is of obvious value. But based on the majority views in
Australia at present it seems that in other circumstances most people will not
benefit from wearing a surgical mask.
General practitioners should be able
to access surgical masks through their local Primary Health Network.
For the latest advice, information
and resources, go to www.health.gov.au
The National Coronavirus Health
Information Line on 1800 020 080 operates 24 hours a day, seven days a week. If
you require translating or interpreting services, call 131 450.
[1]
Those of you old enough to get this joke are hopefully self-isolating at home
and getting your grandchildren to drop groceries at the door.
What is the right thing to do? And how is it best to encourage us all to do it?
An emotive appeal may well have greater impact than a weight
of statistics and numbers. I was inspired by something Amy Remeikis, journalist
with the Guardian Australia, said on ABC TV’s The Drum last week:
“I just hope that when people are walking around and they’re seeing what they’re calling apocalyptic scenes and everyone’s seeing how negative it is; I look at an empty space and I see that as an act of love or of giving, because it’s people trying to save the lives of people they may never meet and that includes my father. – – I know there are people all over the country who are terrified for their relatives and that’s why l really do hope so many people are taking this as seriously as it needs to be taken.”
The Prime Minister and others have consistently attributed decisions
they have made about the virus to the health advice from the Federal and State/Territory
Chief Medical Officers. “Don’t blame or credit us governments; we are simply
following independent, world’s best scientific advice.”
In turn, the Chief Medical Officers have referred to (or deferred to?) the modelling of COVID-19 transmission
and
infection done both here and in other countries.
We
have been promised an open-book approach to the modelling being relied upon,
but have yet to get it. This is perhaps because complete openness would lead to
more distraction from the central task. Those who are already frantic providing
health advice to the National Cabinet can do without debate about their preferred
judgements, including because they differ from those of some other experts.
These
‘others’ include a team from Australia’s leading research universities, asked
for advice by Professor Brendan Murphy, Commonwealth CMO. Their view was not unanimous
but the majority of them called two weeks ago for “a rapid, sweeping and
costly lockdown to pave the way for a national recovery once the crisis
abates”.
Even with open access to the health modelling still more would
be needed in order to understand – and evaluate – the decisions made in
response to the pandemic. Presumably the economic impacts of various potential
decisions have also been modelled, with the inputs being potential decisions
about restrictions on businesses and movement, and the outputs such things as
business turnover, the number of jobs lost and investor confidence.
The third part of the equation, and the most outrageously difficult,
has been to make judgements about the relative value of different outcomes from
the health and economy models. Put simply, it has in effect been a question of
how much economic cost is justified to save a life.
When we have a chance to scrutinise the health and economic
modelling that has been relied upon there will still be disagreement about
whether or not the decisions made have been optimal. One thing we can be sure will
be agreed is that all such modelling consistently displays great sensitivity –
meaning that small changes in the assumptions and inputs at the front end have resulted
in huge variations in outputs. Sensitivity must be even greater where the
phenomenon being modelled is subject to exponential growth.
The Prime Minister has spoken often of the importance of
preserving “life as we know it” – a euphemism for protecting the
economy. For some people it has been impossible to shake the belief that his
and his government’s embarrassment about their premature ‘back in black’
celebrations made them attribute, for some time, more weight to the economic
crisis than to the virus.
In the earliest discussions with my eldest son – rational
and risk-averse – I had taken the (disgraceful?) line that if there is a new
virus in the world we might as well get used to it and develop immunity as well
as we can. On the last weekend before the 500 threshold was declared I was in
Bathurst with about a thousand others at the NSW over-65s hockey championships.
Just in the nick of time.
Soon after that I was a convert to what I think of as The
Norman Swan Line: the government should go hard and early, to maximise the
probability of halting the spread. As Dr Swan has been saying for several weeks,
the only potential down-side of this approach is that if spread is prevented and
nothing happens, the nay-sayers would be able to say that the government had
over-reached. That would be a great outcome!
I have been doing my bit for the Swan line. A sort of epiphany
was at the Parkinson’s singing group on the Monday of the week after the hockey
tournament. As soon as I sat down with the small group of us in the church hall
I realised what we were doing. Given our small number and our recent history of
travel, the probability of our meeting increasing the rate of transmission of
the virus was close to zero. But my decision to attend had contributed to a
meeting – and gatherings of 10 or 500 are occasioned by the individual decisions
of 10 or 500 individuals. The desired outcome cannot be achieved without my
compliance.
We each need to commit to that act of love or giving in order
to save the lives of people we will never meet.
Thus disposed, the staged or gradualist approach adopted by
the National Cabinet “as a result of the medical advice”, never
seemed to me to make sense. If we know that a total lockdown will work, and
that we will probably need that eventually, why wait?
Which brings us back to the modelling of health and economic
impacts. In the case of school closures, the modelling would require assumptions
about different transmission rates with various proportions of school children
at school, based on even more basic assumptions about the behaviour of school
children, parents and the virus itself. The decision to keep schools open while
encouraging parents to keep their kids at home seemed to indicate a lack of
confidence in the modelling and the Federal Government’s unwillingness to be
held accountable for a decision on the matter. The hard decision rested with
the States and Territories.
The Federation seems to have come to the view that the States
and Territories are responsible for action consequent on the belief that overcoming
the health crisis is a pre-requisite to beating the
economic crisis, while the national government acts through its taxing and
spending powers to engage in preparations for economic bounce-back.
The generosity of the national government on economic
matters has been astonishing, although it is people not governments who will
inherit the debt. And it is fervently to be hoped that the cart and the horse
are lined up in the right order.
This piece was published in Croakey on 10 February 2020. It was edited for Croakey by Amy Coopes.
One of the reasons Prime Minister Scott Morrison has given for not bolstering emissions reduction targets is his belief that building resilience for the future is a better way to go.
Speaking to reporters at Parliament House on January 14, this is what he had to say:
I’ve set out what I think we need to do in terms of the future and
that has been very much ensuring that we continue to meet and beat the
emissions reduction targets that we’ve set. I’ve said, though, I think
more significantly that resilience and adaptation need an even greater
focus.
The practical thing that actually can most keep you safe during the
next fire or the next flood or the next cyclone are the things that most
benefit people here and now… The emissions reduction activity of any
one country anywhere in the world is not going to specifically stop or
start one fire event but what the climate resilience and adaptation work
can do within a country can very much directly ensure that Australians
are better protected against what this reality is in the future.
We must build our resilience for the future, and that must be done on
the science and the practical realities of the things we can do right
here to make a difference.”
His address
to the National Press Club on January 29 featured 16 references to
‘resilience’. They included an assertion about the economy’s resilience,
resilience to natural disasters, to a changing climate, and to
unspecified other threats. He spoke of national resilience, practical
action on climate resilience and adaptation, and asserted that
mitigation and adaptation both contribute to resilience.
Farmers, he said, are on the frontline of resilience.
“The $5 billion Future Drought Fund will support practical,
resilience-building measures, including small-scale water infrastructure
and improved information on local climate variability, sustainable
stock management, soil and water regeneration and the like. Our Drought Resilience Funding Plan
— the framework to guide funding decisions for projects and activities —
is expected to be tabled in Parliament by March of this year,” he said.
The Reef 2050 Plan
and investments in “the technology of resilience, science of resilience
through agencies such as the Bureau of Meteorology, the CSIRO and the
Bushfire & Natural Hazards CRC” were among other measures touted by
the Prime Minister in his address.
Looking ahead, he said he had tasked the CSIRO with bringing forward
recommendations, supported by an expert advisory panel chaired by
Australia’s chief scientist, on “further practical resilience measures,
including buildings, public infrastructure, industries such as
agriculture, and protecting our natural assets.”
Added Morrison:
I will be discussing resilience measures with the states and
territories at COAG in March, and I know they’re looking forward to that
discussion, including to ensure the Commonwealth Government’s
investment through the National Bushfire Recovery Agency will be in
assets that are built to last, built to resist, built to survive longer,
hotter, drier summers. Building Back Better for the future.”
But what exactly is this ‘resilience’ of which much is expected? Do
we all share a common view of what it is, what it does, and how more of
it can be created?
the power or ability to return to the original form, position, etc., after being bent, compressed, or stretched; elasticity.
ability to recover readily from illness, depression, adversity, or the like; buoyancy.
The first thing to note is that ‘resilience’ is a positive thing – an
asset. In this particular definition, resilience is a power or an
ability.
When applied to a physical entity, resilience refers to its capacity
to return to original shape, following the application of external
pressure. In such a case, resilience is attributable to the properties
of the substances of which the entity is made.
The extension of this notion to human communities is easy and
pleasing. The individuals in the community are the constituent parts,
akin to the molecules that provide a substance with its physical
properties. The property of a particular community with respect to
resilience is determined by the individuals in it, the relationship
between them and their aggregated response to an external force.
There is a large and rich literature on community and personal
resilience, traversing disciplines such as psychology, sociology,
engineering, geography and management.
One systematic literature review
of definitions of community resilience related to disasters published
in 2017 found no evidence of a common, agreed definition. It did,
however, identify nine common core elements of community resilience.
They are:
local knowledge
community networks and relationships
communication
health
governance and leadership
resources
economic investment
preparedness
mental outlook
The study notes that due to climate change and demographic movements
into large cities, disasters are occurring more frequently and in many
cases with higher intensity than in previous years. This has prompted a
stronger focus on how best to help communities to help themselves, with a
concomitant focus on understanding what factors contribute to making a
community resilient to disasters.
The authors write:
The concept of ‘community resilience’ is almost invariably viewed as
positive, being associated with increasing local capacity, social
support and resources, and decreasing risks, miscommunication and
trauma.
Yet consensus as to what community resilience is, how it should be
defined, and what its core characteristics are does not appear to have
been reached, with mixed definitions appearing in the scientific
literature, policies and practice. This confusion is troubling.
The way we define community resilience affects how we attempt to measure and enhance it.”
So community resilience is something that cannot be identified at a single point in time, but over time — in particular over the period after a community has been exposed to pressure.
How did the community respond? Did it return to its original shape, form and pattern of behaviour?
Resilience located
People who live in communities that can rebound are the lucky
ones.The lives of many others are characterised by pressure and
deprivation, but without the resources (the skills, financial means,
information, personal health etc) and equitable access to the supports
required to bounce back.
There are a number of educational resources relating to the fostering of resilience. One has it that the seven Cs of resilience are competence, confidence, connection, character, contribution, coping, and control. Another asserts that resilience is made up of five pillars: self awareness, mindfulness, self care, positive relationships and purpose.
The 5 Pillars of Resilience. Image credit: The Wellness Project
I am familiar with the term and its application from my time working for the National Rural Health Alliance as a rural advocate. One of the purposes of that work was to try to ensure that rural issues were ‘on the agenda’.
This season’s bushfires
have thrown the public spotlight on rural and remote areas like almost
never before, also highlighting the community spirit which commonly
exists in them. We have been reminded daily of the devotion of
individuals who serve rural communities so expertly and selflessly: in
rural fire services, the SES, Shire Councils, charitable organisations,
the State and Federal public service, and many other bodies.
Though not exclusively a rural phenomenon, this sense of community — a
key ingredient for resilience — seems to flourish more easily or more
frequently in rural areas, so much so that community spirit is often
said to be one of the features distinguishing rural from city living.
‘Community’ flourishes where human networks are small and open,
making for rapid communications and visible personal circumstances.
Local communications were perhaps always more efficient and
comprehensive in rural areas due to partyline phone services and an
effective bush telegraph, roles now largely adopted by social media.
The visibility of personal circumstances is not always a positive
thing. It is a major contributor to stigma, which inhibits help-seeking
in rural areas among some population groups in some circumstances.
The prosaic signs of community spirit and connectedness include a
willingness by people to roll up their sleeves and get involved in work
towards a shared local purpose; a can-do attitude witnessed in spades
over recent months, with some local communities already rebuilding in
earnest.
Occasionally, though, we should perhaps pause and consider the
possibility that replication of patterns and structures that existed
before the firestorms may not represent resilience. Such a return to the
status quo may run counter to the adoption of new, more desirable,
regulations relating to such things as where houses are built, how they
are constructed, and what fire precautions are required. Not just
building back, but Building Back Better, as framed by the government.
When the fires are out and the rebuilding is underway, it is to be
hoped that the public and its governments maintain an appropriate focus
on the communities of rural and remote Australia. It is vital that they
do so because the conditions that exist — not just in times of crisis
but in good times as well — are in some respects quite different from
those in the major cities, requiring policies and programs that fit.
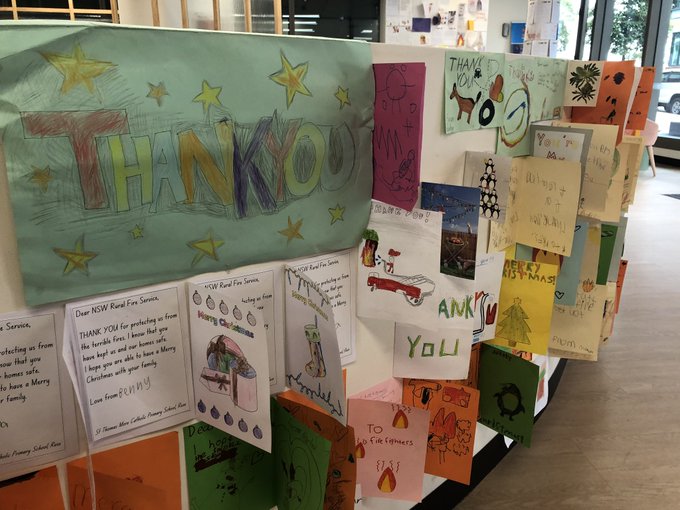
Thank you cards for NSW firefighters in the foyer of the Rural Fire Service HQ, Sydney. Image credit: Sascha Rundle
Resilience enhanced?
Rural communities do not need or want to always be seen through a
deficit lens. Despite the real and ongoing challenges they face, people
from rural and remote areas frequently score higher on self-perceived
notions of ‘happiness’. It is not clear what the main reasons for this
are, but they are likely to include the benefits of a stronger sense of
community.
However there is a risk involved in this. Greater community
connectedness must not be seen as an alternative to or replacement for
services provided by governments and paid for from the public purse.
Resilience is not a reason to let governments off the hook as service
providers whose challenge is providing equivalent access to such things
as health, education, broadband or aged and disability services to
people in all parts of the nation.
It’s not as if resilience and public services are a zero-sum game.
And rural people want to be thought about and properly considered in
good times as well as bad.
Given the local, spontaneous, community-driven nature of resilience,
the active involvement of the government in enhancing it may be
ambitious or even counter-intuitive. If it is to proceed as the Prime
Minister has indicated, there needs to be an agreed definition of what
it is, and agreed measures to quantify its existence. It should be
possible to design research which will meet the need for both agreed
definitions and empirical research on its existence and effectiveness in
various locations.
When defining resilience some of the urban (and rural) myths must be
exposed. Rural males have sometimes been thought of as ‘resilient’
because of their unwillingness to see a doctor or to care for their own
health in other ways. This is to confuse resilience with pride, risk
aversion and fear.
Health services in rural areas — although stretched by large
distances, higher costs and workforce shortages — must be prepared to
meet the challenges posed by environmental disasters such as floods and
fires, animal-borne infections, and epidemics. The responses of health
agencies during the bushfires will be a matter for consideration once
the emergencies have passed. And, unfortunately, those same health
services may soon be tested in relation to a new epidemic.
It may be short of resources, but in a cultural sense Australia’s
rural health sector is well-equipped for disaster management. It has a
strong values base, centering universality, equity and compassion.
Resilience is a second-best approach
The systematic review quoted earlier drew a very practical conclusion:
“In spite of the differences in conception and application, there are
well understood elements that are widely proposed as important for a
resilient community. A focus on these individual elements may be more
productive than attempting to define and study community resilience as a
distinct concept.”
And what of the choice between disaster prevention and enhanced resilience?
Of course it’s not either/or, but given a choice between disaster
prevention and resilience, any rational being would choose the former.
The best bet is to be without adversity and unhappiness in the first
place.
Occasionally since the May 2019 election people have wondered,
rhetorically, just how quiet the Prime Minister wants Australians to be.
It is to be hoped that the Quiet Australians — whoever and wherever
they are — appreciate the basic after-the-event connotation of
resilience, and do not allow it to displace or reduce Australia’s
efforts to minimise carbon emissions.
It’s more important and more rational to prevent the need for a community to rebound than to enhance its ability to do so.
Climate change ‘resilience’ must not be allowed to morph into climate change ‘silence’.
The bushfire emergency has transformed understanding of the facts relating to climate change and its impact on weather events. What was hypothetical has become personal.
Flinders Chase National Park after bushfires swept through Kangaroo Island, South Australia. Photograph: David Mariuz/AAP
People
living in rural and remote areas of Australia have always felt the brunt of
extreme weather events such as bushfires, cyclones and floods. Therefore increases
in the frequency and intensity of adverse weather events have, until now,
constituted rural issues. It has been
difficult to have them treated as ongoing top national priorities.
But suddenly
understanding about them has become national because of the spatial and
temporal extent of the emergency. Also, some of the impacts, such as smoke
haze, have been experienced directly by people in the cities for an extended
period.
At 3.00pm on 8 February 1983 about 1,000 tonnes of Mallee topsoil were dumped on Melbourne. It was reported that “city workers huddled in doorways, covering their mouths from the choking dust, and traffic came to a standstill”. The worst of the dust storm was over by 4:00pm, when the wind speed dropped.
Melbourne, 3.30pm Tues.8 Feb. 1983
For a few
days the significance of drought and the conditions that caused it were no
doubt a topic of conversation in Melbourne. Tragically the exact weather
pattern that had caused the dust storm in the city that day was repeated one
week later, when the Ash Wednesday fires caused enormous destruction. In Victoria and South Australia 75
people died, including 17 fire-fighters.
"Australia’s weather and climate continues to change in response to a warming global climate. Australia has warmed by just over 1°C since 1910, with most warming since 1950. This warming has seen an increase in the frequency of extreme heat events and increased the severity of drought conditions during periods of below-average rainfall. Eight of Australia’s top ten warmest years on record have occurred since 2005." [1]
"- - very high monthly maximum temperatures that occurred around 2 per cent of the time in the past (1951–1980) now occur around 12 per cent of the time (2003–2017). Very warm monthly minimum, or night-time, temperatures that occurred around 2 per cent of the time in the past (1951–1980) now also occur around 12 per cent of the time (2003–2017). This upward shift in the distributions of temperature has occurred across all seasons, with the largest change in spring."
One of the
underlying causes of the current bushfire emergency has been the long-term and
extensive drought. Once the immediate recovery of people, their communities and
their businesses is in full train, it will be essential to return to
consideration of policies relating to the management of water and drought, and
the management of land and agriculture.
These are
very complex policy areas as illustrated, for example, by the unavoidable
conflicts in water policy between state and territory jurisdictions, between
economic, domestic (household) and environmental purposes, and between
individual end-users.
Because of
long-term basin-wide rainfall shortages, the Murray-Darling Basin Plan, the
result of a huge amount of expertise, negotiation, good will and compromise, signed
into law in 2012, now stands accused and unloved like a convicted thief in an
open court.
"The year-to-year changes in Australia’s climate are mostly associated with natural climate variability such as El Niño and La Niña in the tropical Pacific Ocean and phases of the Indian Ocean Dipole in the Indian Ocean. This natural variability now occurs on top of the warming trend, which can modify the impact of these natural drivers on the Australian climate."
National uncertainty
about how best to manage waters, land and weather has been compounded by global
warming. The adverse effects have been worse for people in rural areas, who face
some immediate challenges and disadvantages not experienced equally by people
in the cities.
A
description of the population characteristics of those who are most vulnerable
to the adverse effects of severe weather events fits like a glove for rural
people. They are those who are isolated, are of poorer socio-economic status,
have pre-existing health conditions, have less access to infrastructure for
transport, heating and cooling, fresh water and food; and have limited access
to timely and appropriate health services.
About
two-thirds of Australia’s Aboriginal and Torres Strait Islander people live
outside Australia’s major cities. As a population group they have significantly
poorer health outcomes, which makes them
especially vulnerable to the adverse effects of weather events.
A Fact Sheet
from the National Rural Health Alliance says in part:
"Hospitalisation rates for asthma and chronic obstructive pulmonary disease (lung diseases that prevent proper breathing) are already substantially higher in remote areas, and this is likely to be exacerbated by warmer temperatures, coupled with elevated levels of airborne pollens and pollutants, such as bushfire smoke. Homes in rural and remote areas are older and often lack the thermal efficiencies of newer homes (e.g. reflective roofing and insulation). Aged care facilities in rural areas are also generally older, smaller and hotter than those in urban facilities."
There is,
however, good news and some of it could be set in place with less contested
policies and programs than those that relate to drought and water management.
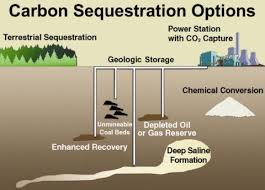
The business sector the world over is already responding to the price signals and new commercial opportunities that are emerging as part of activities to reduce global warming. The largest and most immediate commercial opportunities include further developments and growth in the renewable energy sector, and carbon sequestration – the long-term storage of carbon in plants, soils, geological formations, and the ocean. In his recently-published book, Superpower, Ross Garnaut asserts that carbon sequestration could capture up to 1 billion tonnes a year – nearly twice Australia’s annual emissions.
This and much
else of the economic adaptation required to reduce per head emissions and
global warming will necessarily be based in rural and remote areas. This means
that, just as the adverse effects of climate change and weather events are felt
most immediately and extensively in rural and remote areas, so are the economic
opportunities.
Our political
and business leaders, small and large, should make more of the positive
differential for the economic development of non-metropolitan areas inherent in expanding and new ecologically-enhancing
industry sectors.
Ross Garnaut
has been the author of advice to governments on climate change for many years.
He has no doubt that renewables can meet
100% of Australia’s electricity requirements by the 2030s, with high degrees of
reliability and at lower prices. He says that embracing low-carbon
opportunities could lead to a clean electricity system more than three times
the existing capacity that powers a transformed economy, including electric
transport and new and expanded industries in minerals smelting.
The dramatic
decline in the cost of renewable energy has brought forward by a decade the
time when cheap wind and solar power could provide the country with an
advantage in energy-intensive manufacturing. Along with the expected
development of green hydrogen, it could help make Australia a natural home for
expanded industries in aluminium, steel, silicon and ammonia.
The crucial thing for the people and business of rural areas is that these industrial opportunities will underpin growth and jobs in regional centres such as the Pilbara, the Upper Spencer Gulf in South Australia, Portland and the Latrobe Valley in Victoria, Newcastle in NSW, Townsville, Gladstone and Mackay in Queensland and parts of Tasmania. This would help transform the economy and future prospects of rural areas.
A renewable rural economic base
Note: The NRHA has published (6 January 2020) a list of resources for people in bushfire-affected communities. (Accessed at https://www.ruralhealth.org.au/news/resources-people-bushfire-affected-communities). It includes advice on preparing children for the psychological effects of bushfires, on personal recovery, the provision by pharmacists of medications, avoiding harm from smoke, mental health, some phone lines for assistance and some regional data sources.
[1] The figures quoted in this piece are from State of the Climate 2018, CSIRO BOM, Dec. 2018; accessed at https://www.csiro.au/en/Showcase/state-of-the-climate
Brexit (/'breksit, breqzit/; a portmanteau of 'British' and 'exit') is the withdrawal of the United Kingdom (UK) from the European Union (EU). Following a referendum held on 23 June 2016 in which 51.9 percent of those voting supported leaving the EU, the Government invoked Article 50 of the Treaty on European Union, starting a two-year process which was due to conclude with the UK's exit on 29 March 2019—a deadline that has been extended to 31 October 2019. [From Wikipedia, the free encyclopedia]
It’s none of my business. But I have a strong emotional attachment to something called the United Kingdom.
Why on earth would Boris Johnson commit to leaving the European Union on October 31 – “No ifs, no buts” – on the basis of a decision made by the people over three years ago?
Such a dogmatic approach to an outdated electoral outcome makes no sense.
Tying oneself to yesterday’s facts is neither admirable nor principled; it is ideological.
Keynes may or may not have said “When the facts change, I change my mind. What do you do, sir?”. Irrespective of the accuracy of this famous attribution, it’s a fine and robust idea. Matters of fact should be determined by the best information. And the best information must include the most recent.
Surely ‘the statute of limitations’ has been reached for a decision made over three years ago? For goodness sake: in Australia, three years is longer than the average term of an elected parliament! There’s no way we would have our Parliament peopled by candidates who were successful in the election before last.
Rory Stewart, who flared brightly and briefly in the Conservative party firmament in recent months, made a case for not having a second referendum. He pointed out that, should the decision be reversed, the Leave forces would take to the streets immediately and there would be no end to the schism.
But even if that were the case, at least the divisiveness would be based on up-to-date information! And there might be every chance that the case to remain in the EU would be better than 51.9%. The demographics have shifted in favour of the remain vote. There is now much greater clarity about what leaving means in terms of trade and jobs, and what the practical difficulties are.
And surely a significant proportion of those who voted leave would agree that they did not vote for the uncertainty and bedlam of the last three years?
There are only three options: to leave subject to the agreement reached with the EU; to leave with no agreement; or to call the whole thing off. Maybe those could be the choices in a second referendum.
Respecting the primacy of the people and their vote is the essence of democracy. But it is false logic and dysfunctional to be tied to historical decisions of the people which, in all probability, no longer hold.
And there is one way to be absolutely sure. Ask them again.
Post script: in an interview with James O'Brien, and asked whether he thinks Boris Johnson is "dangerous", Rory Stewart paused for 11 seconds before answering. There was an earlier and revealing discussion between the two on O'Brien's LBC radio show.
When politicians treat us like mushrooms, what do we need to know?
Health electioneering is a minefield, with almost limitless possibilities for the public to be misled and bamboozled. We need more than a Charter of Budget Honesty to stop the rot.
Politicians should be required to provide enough detail of their claims about costs and benefits for the facts to be clear to everyone. And the important next step is to have the policy debate about which assumptions or definitions are better for the nation – and why.
In the early days of the federal election campaign, the public suffered a welter of claim and counterclaim from the major parties about dollar figures for intended and unintended cuts, and about the cost and benefit of existing and proposed programs.
Some of the disputes are academic in the sense that they relate to projections for future periods beyond two elections. Others are critical for the next period of government, and evaluation of them should therefore be part of voting decisions made.
One of the main areas of such disputation in the health sector is the funding of public hospitals. A piece [https://bit.ly/2vo16Mf] in Croakey by Stephen Duckett explains how it is that, given certain assumptions and interpretations of what the word ‘cut’ means, both the Government and the Opposition are ‘right’ about public hospital funding.
Once the ambiguity is explained, the desirable next step is for the public to make a judgement about which position on the matter is better.
What difference to hospital services (waiting lists, quality and safety, patient-centredness etc) do the Labor and LNP funding commitments make (50 and 45 percent of the growth in public health costs respectively)? It is incumbent on both sides to press the claim for the policy that underpins their definition, otherwise it is just another academic dispute.
This dispute about hospital funding is a specific case study of a phenomenon too-much-loved of both sides of politics: using selective language and the complexity of budget processes to keep the public in the dark.
This article examines some of the general budget processes which need illuminating, including those relating to open-ended demand-driven programs that are at the heart of Australia’s health system.
Even more important than the existence and size of ‘budget black holes’ are the policy choices and narratives that lie behind the numbers.
Selective inclusion and definition
As has been explained elsewhere, conflicting dollar figures about ‘cuts’ can arise simply because of the selection of different things to measure and through the attribution of particular meaning to words like ‘cuts’. The context for different claims is the quite complex system of Federal Budgets, and both sides of politics can benefit from a continuation of the misunderstanding so are not always disposed to clarify matters.
The difficulty for the public in getting to the bottom of dollar figures is not restricted to cuts.
There is also uncertainty about the dollar amounts promised for programs newly announced, especially in an election campaign when promises come thick and fast. It is often impossible to be sure whether new money would be involved or whether there is double counting or reconfiguring or re-branding of existing allocations.
As an example, no-one could object to the notion of extra investment in preventing suicide among young Aboriginal and Torres Strait Islander people. But it is an impossible challenge for all but the public servants and advocates immediately involved to know how much of ‘the $461 million Youth Mental Health and Suicide Prevention package’ would be new and how much would be money shifted around, renamed and re-announced.
Promises concerning new programs like this are, in any case, hypothetical unless and until the promising party is elected to government.
What is meant by ‘Budget cuts’?
There are three main forms of ‘Budget cut’:
a reduction in an absolute dollar amount allocated for a particular purpose;
an increase in the amount allocated that is less than the previous year’s plus the amount needed to allow for inflation (“a cut in real terms”); and
an allocation that is less than was previously foreshadowed in a forward budget estimate.
This last is important in the health sector. It is properly described as a cut in projected spending growth.
Cuts in projected spending growth
Let us assume that the dollar allocation in the current financial year to a particular purpose is 100 dollar units.
The standard budget structure requires the government to indicate its intentions with respect to the funding of that particular purpose for the next four financial years. If it is anticipated that this ‘particular purpose’ will remain of the same order of priority, the Budget might forecast allocations to it of 103, 106, 109 and 113 units in each of the four coming years (Table 2).
This status quo may be retained, or there may be decisions made which mean that actual allocations in years 1-4 are different from what was proposed at Year 0.
For example, it is possible that serious fiscal pressure (for instance in order to meet the promise of a projected budget surplus) might result in the program being cut. In Year 1 only 102 units are spent and the allocations to the four ‘out years’ are changed to 104 (rather than 106), 106 (not 109), 110 (not 113), and 112 in the new fourth year. Such changes could be described as a cut of 9 units against forward estimates [(3+6+9+13) minus (2+4+6+10)].
Alternatively, changes to the projected allocations may be driven by external shocks which work in the other direction to increase expenditure.
For instance, it might be a drought support or recovery program. Suppose that in Year 1 there is a shocking and widespread drought. For that year 103 units were originally allocated. The extent of the drought that year demands the allocation of substantial additional money. Cabinet decides to spend 106 in the current year and in that year’s Budget it decides to increase the allocation for Year 2 to 110.
That Budget will also project the allocation for Years 3, 4 and 5. The Government’s approach to drought policy will be tested and illustrated by the forward estimates it makes.
Will it see drought as a natural event for which there should be a range of plans? Will it provide income support and welfare assistance? Will it act to reduce the adjustment pressure on farms affected by the drought? Will it just pray for rain?
These are the critical options that lie behind the budget numbers and which ought to be the subject of serious informed discussion.
The mystery of Budget forecasts
It seems to be accepted that the allocation of public money to drought programs should be decided from time to time as drought occurs, with the consideration being made each time without any agreed overarching policy framework.
The advantages of this approach include ‘flexibility’ – a term which accommodates political opportunity. Its disadvantages include the lack of predictability and certainty which could underpin longer-term national, state, regional and property-level planning for drought.
Health expenditure and demand-driven programs
The flexibility and uncertainty inherent in a program area like drought do not exist in many other areas of major expenditure, including some in the health sector. This is because expenditure in those programs is open-ended and ‘demand-driven’.
Two of the largest programs funded by the Commonwealth in the health sector are of this type. They are the Medicare Benefits Schedule (MBS) and the Pharmaceutical Benefits Scheme (PBS). Decisions about the amount spent through these are less easily managed or altered by the government of the day.
Between them the MBS and PBS cost the Federal Government (2016-17) $45 billion, or 61 percent of its total spend on health. Both are open-ended (ie unlimited) demand-driven programs. Each has a set of regulations through which eligibility for a payment is established as well as the amounts paid in all circumstances that might exist.
Demand-driven programs have momentum (mass x velocity), like a tanker at sea; the Government can alter the course (cost) of these programs slightly through changes to the criteria that apply. But large changes in direction are in effect ruled out because of the foundational principles represented in the programs, and thus by political risks.
Suppose that through the Commonwealth’s due process, a new pharmaceutical is added to the PBS. The Commonwealth becomes liable for providing that pharmaceutical to as many consumers as are prescribed it – perhaps only in certain specified circumstances (for example for one particular clinical condition but not others).
The same general process determines expenditure under the MBS. New activities (‘items’) are added to the Schedule and become eligible for payment and, very occasionally, existing items become ineligible.
(There have been great expectations of the current MBS Review in this latter regard. There are over 5,700 MBS items and the Review Taskforce is charged, among other things, with the identification of items that are obsolete, outdated or potentially unsafe. It has established over 70 Clinical Committees to provide it with expert advice.)
Remember this?
One of the more infamous attempts to re-chart SS Medicare’s course was when Nicola Roxon, armed with information about how the procedure had been transformed (simplified) by technology, tried to halve the schedule fee for cataract surgery.
Eventually the Minister failed in her clear-sighted intention; but the compromise deal agreed in the Senate did include $5 million in a separate fund to offset costs of cataract services for Indigenous and rural patients.
The freeze on rebates for GP services under the MBS, introduced by the Labor Government in 2013 and retained under Abbott, Turnbull and Morrison, was a temporary re-design of the system that has saved the Commonwealth perhaps $2 billion – and increased out-of-pocket costs to patients. The freeze is being removed in stages.
Another demand-driven program currently in the public eye is the National Disability Insurance Scheme (NDIS).
The forward estimates of what it would cost the Commonwealth have not been met due to some mixture of bureaucratic stasis or incompetence, poor management, lack of consultation, over-ambitious expectations and/or secret bloody-mindedness.
The misery caused by the NDIS’s failure to take shape as quickly as anticipated has been given greater public attention than might have been the case because of the underspend’s contribution to a forecast Budget surplus next year (2020-21).
A Charter of Policy Honesty?
Conflicting claims in election campaigns about one party’s intentions to cut programs or about the cost of promised new initiatives continue to irritate the public. Judgments about ‘budget black holes’ have won and lost elections a number of times.
Progress has been made with the Charter of Budget Honesty, enabling the Departments of Treasury and Finance to cost election commitments during the caretaker period. However, if the costings relate to policy proposals that are mired in uncertainty due to a lack of detail or selective interpretation, the public is still not properly informed.
Politicians should be required to provide enough detail of their claims about costs and benefits for the facts to be clear to everyone. And the important next step is to have the policy debate about which assumptions or definitions are better for the nation and why.
A Charter of Budget Honesty is one thing; the policy choices and narrative behind the numbers are even more important.
This piece was first published on 20 March 2019 in Croakey.
In recent considerations of out-of-pocket health care costs, we seem to have forgotten the flamin’ obvious: th costs associated with unavoidable travel to a service aren’t being considered at all.
Neither the Report of the Ministerial Advisory Committee on Out-of-Pocket Costs (November 2018) nor any of the media commentaries I have found about it include a single reference to the words ‘rural’ or ‘transport’.
Gordon Gregory
It’s a worry if we are so blind or indifferent to the realities of rural living that no consideration is made of how different out-of-pocket costs are in more remote areas, and how different the options for remediation are compared with major urban centres.
Are we surprised? The committee comprised representatives of nine specialist medical colleges and six others – and zero representatives specifically of rural and remote people.
The good, the bad and the hopeless
People with health conditions requiring a consultation with a GP, a dentist or a medical specialist can be divided into three groups: the good, the bad and the hopeless. I reckon that in major urban centres in Australia the proportions in these categories are 60:30:10. In more remote areas I reckon it’s 10:30:60. Let me explain.
In the good category are people who have a working telephone, a car of their own or a train station nearby, and sufficient financial means to phone up, make an appointment and subsequently meet it.
The bad have somewhat compromised access to the required health service for a range of reasons. Some – for technical, financial or personal reasons – have imperfect communications. Some can’t afford a babysitter or time off work, or don’t have the confidence to travel in public. Some can’t afford to pay the out-of-pocket cash costs of the consultation, many of them because they have no private health insurance.
People find themselves in the hopeless category because of the inability to pay the total cost of accessing a service, and a lack of information and poor communications systems, and logistical challenges relating to their workplace and location – and no private health insurance.
The attention being given to this matter is on costs of a particular kind and how to improve the value of private health insurance.
Bias against rural and remote people
The definition of out-of-pocket costs being used is the difference between a fee charged for a health treatment or service, and the combined Medicare and private health insurance benefits for the service. It does not include the amount the patient pays in unavoidable ‘ancillary costs’, chief among which are for transport and accommodation. The whole exercise is therefore biased against people in rural and remote areas.
Given two families of the same size and of the same financial means, in every case it will be the one that lives in a rural area that faces the higher financial hurdle in getting a service.
Rural GPs are a proud and generous lot and will try to bulk bill patients of theirs who they feel warrant it. Rates of bulk billing tend to be a bit lower in regional areas than cities, but a bit higher in very remote areas. But the generosity or compassion of an individual doctor should not be the determining factor in whether or not a patient gets medical care.
It is the rural family that will have to spend the most time away from home when they have an appointment with a specialist, necessitating family back-up for a longer period. Specialist clinics, like more specialised hospitals, still pay little heed to the logistical requirements of people who have travelled from distant areas to keep an appointment with them.
The focus of the report’s terms of reference on private health insurance was pretty unappetising for rural people anyway. About 40% of people in outer regional areas have private health insurance. in inner regional areas it’s 50% and in the major cities 61%.
Subsidies useless where private health not available
Government subsidies related to private health insurance are useless to people living in areas where private health is not available. In major cities there are about 175 separations per 1000 people from private hospitals, compared with 67 per 1000 in very remote areas .
And let’s not forget the skewed premise for private health insurance rebates in any case. The ABS’s Australian Social Trends 2010 reminded its readers that:
‘People living in the most disadvantaged areas reported much lower rates of private health insurance than those living in the least disadvantaged areas (28% compared with 75%). As the relative disadvantage of areas decreased there was a clear increase in the proportion of people who had private health insurance, rising from 43% to 50% to 61% across the three middle quintiles. This pattern is not surprising given the government policy to encourage people who can afford private health insurance to take it out.’
The recent report from the Ministerial Advisory Committee reminds us that ‘consumers can be faced with large and/or unexpected costs; this can cause financial hardship and contribute to a perception that private health insurance provides poor value for money.’ I wonder if there was talk around the table of journeys to health care appointments that began with a barge trip to the mainland followed by two legs of a plane trip to the nearest city in which the service was available.
These extra access difficulties are important. The initial presentation by a rural patient in the course of illness is often later than the standard for a patient living in a major city. This has serious clinical implications for the effectiveness of treatment and care, and thus for patient outcomes.
Answers
What are the answers? Policy remediation can be by four means:
having private health insurance providers offer additional products designed specifically to appeal to people in rural and remote areas and to meet their circumstances – including their need to travel and the possibility of significant lost income;
redesigning the system of incentives and penalties relating to families’ decisions about whether or not to take out private health insurance, as the current system of health insurance rebates is another transfer payment from rural to urban populations;
redesigning the system of rebates through both private health insurance and Medicare benefits to accommodate the fact that some people have unavoidable ancillary costs of access; and
governments continuing to make special provision for primary care health services in rural and remote areas, including through workforce training and retention programs.
The last of these is hopefully locked in for good. The other three seem to be missing in action.


























 It seems to be accepted that the allocation of public money to drought programs should be decided from time to time as drought occurs, with the consideration being made each time without any agreed overarching policy framework.
It seems to be accepted that the allocation of public money to drought programs should be decided from time to time as drought occurs, with the consideration being made each time without any agreed overarching policy framework.

